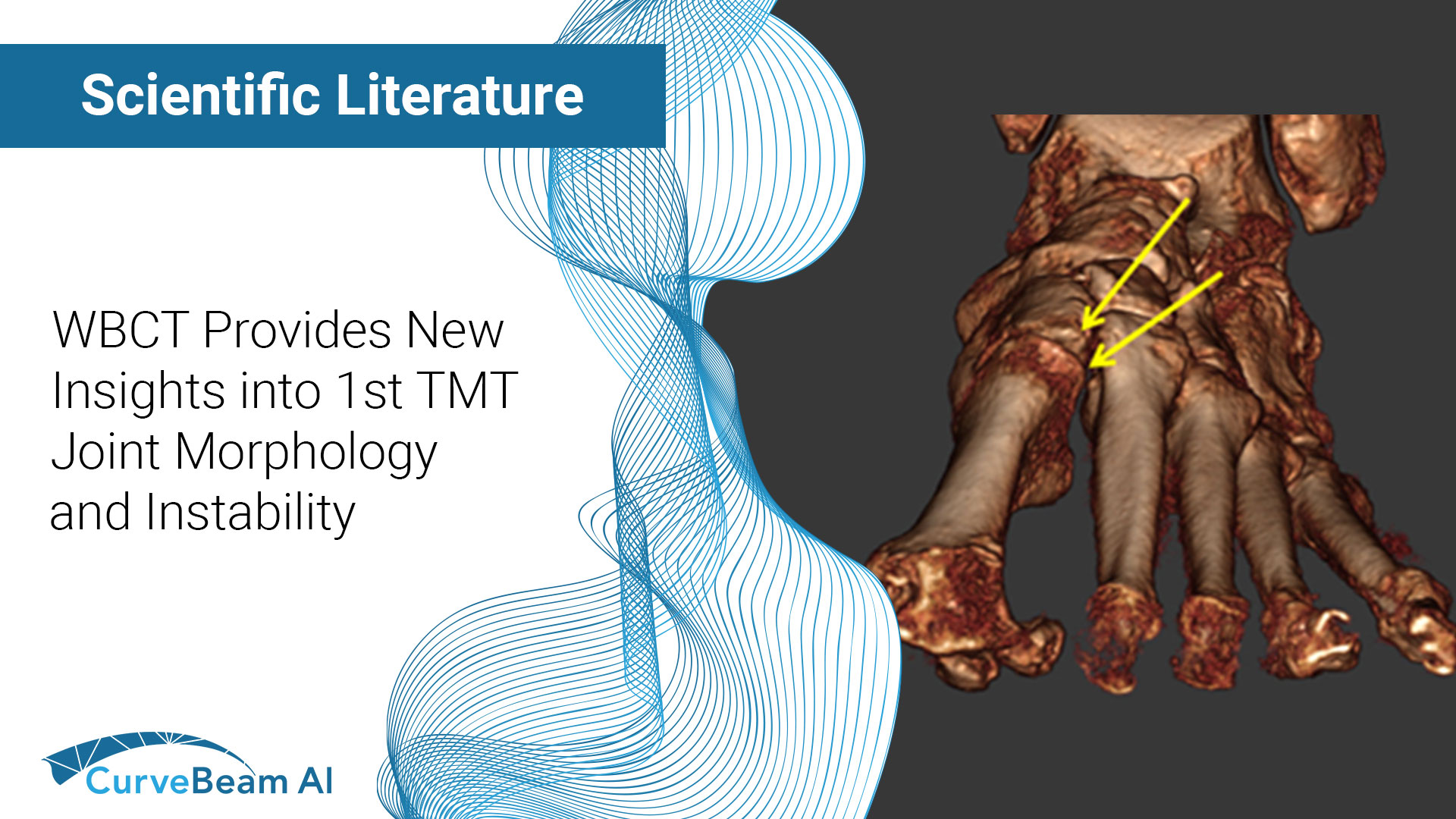
Key Points: First tarsometatarsal joint (TMT1) hypermobility is associated with hallux valgus (HV) which is…

WBCT and its Evolving Role in OA Research and Clinical Practice
Key Points:
- Weight bearing CT (WBCT) can detect signs of osteoarthritis (OA), such as osteophytes, subchondral cysts, and joint space narrowing better than radiographs.
- Emerging evidence suggests WBCT reveals meniscal extrusion not detected by MRI and WBCT arthrography visualizes meniscal tears.
- In clinic, WBCT could expedite diagnosis and treatment of knee OA by identifying which patients are most likely to benefit from bracing surgery, and other biomechanical therapies.
Osteoarthritis (OA) is increasingly becoming more prevalent with the rise of an aging population, creating a need for more sensitive and accurate imaging modalities to assist in diagnosis and monitoring.
The current standard of care for OA diagnosis is standing fixed-flexion radiography (FFXR), but this is a limited test that cannot look at the 3D bone structures, 3D joint spaces, menisci, cartilage, ligaments, muscle or other soft tissues. Non-weight bearing (NWB) 3D imaging such as CT or MRI improves visualization and diagnostic performance for multiple joint tissues, but the imaging is not performed while the patient is weight bearing.
Unlike NWBCT or NWBMRI, weight bearing CT (WBCT) gives a 3D look at the physiological stresses on the cartilage and menisci in the knee. WBCT systems, such as CurveBeam AI’s HiRise, have narrowed the gap left by MRI and FFXR by offering higher sensitivity, accuracy, and predictive values for detecting osteophytes and subchondral cysts which are the hallmarks of knee OA. WBCT also visualizes the alignment of the tibiofemoral and patellofemoral joints (which are not seen on NWBCT or NWBMRI). (K.Kaneda et al. MNC Musculoskelet. Disord 23 (1) (2022) 253)
Researchers at the Department of Rehabilitation Medicine, University of Kansas Medical Center, Kansas City, KS, looked at research from the past 15 years and outlined the evolving role WBCT has played in evaluating OA:
Joint Space Width & Joint Space Mapping
Although knee joint space width (JSW) on FFXR is the most common measurement for cartilage loss, it is often overestimated on radiographs, leading to incorrect grading of OA. In addition, JSW does not decrease uniformly across the joint. WBCT can evaluate each region of the joint separately via multiplanar reconstruction slices. Because of this, WBCT could be key in the early detection of knee OA. (Segal et al. Phys. Sportsmed. 43 (3) (2015) 213-220)
JSW mapping has historically been performed manually, and can suffer from operator error. However, JSW mapping on WBCT has recently been automated, and accurate results can be available immediately.
Meniscus Evaluation
WBCT arthrography (WBCTa), WBCT enhanced with intra-articular injections of iodinated contrast agents, enables visualization of patellofemoral cartilage that cannot be seen on MRI. WBCTa displays meniscal extrusion and meniscal tears not seen on FFXR and even demonstrates higher grades of extrusion than on MRI. (Segal et al. Proceedings of the Orthopaedic Research Society 2021 Annual Meeting, 2021 2/13/2021)
OA Case Management
Finally, having WBCT in clinic could expedite the diagnosis and treatment of knee OA by identifying which patients are most likely to benefit from bracing, surgery or other biomechanical therapies. Multiplanar reconstructions of the knee, hip and ankle from any angle could improve pre-operative planning and post-operative assessment of functional alignment following procedures such as distal femoral osteotomies, proximal tibial osteotomies, unicompartimental knee arthroplasty, and total knee arthroplasty.
For a full list of the research papers examined and to read the full study click here.
Related Posts